Understanding Carotid Disease
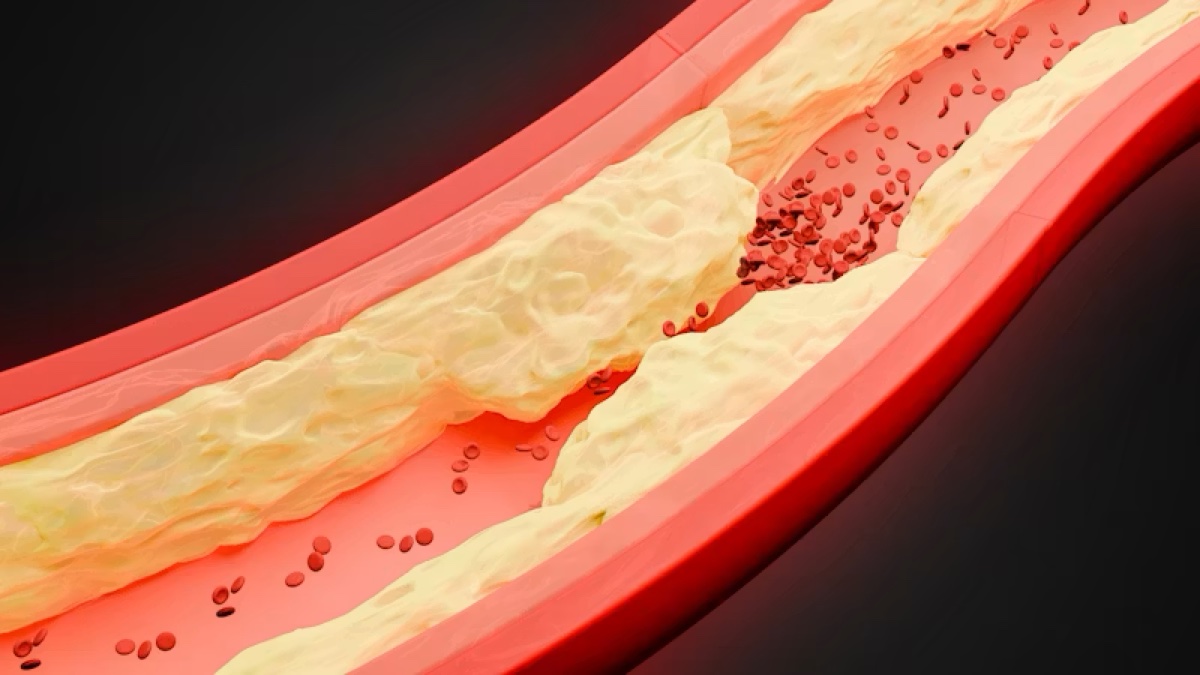
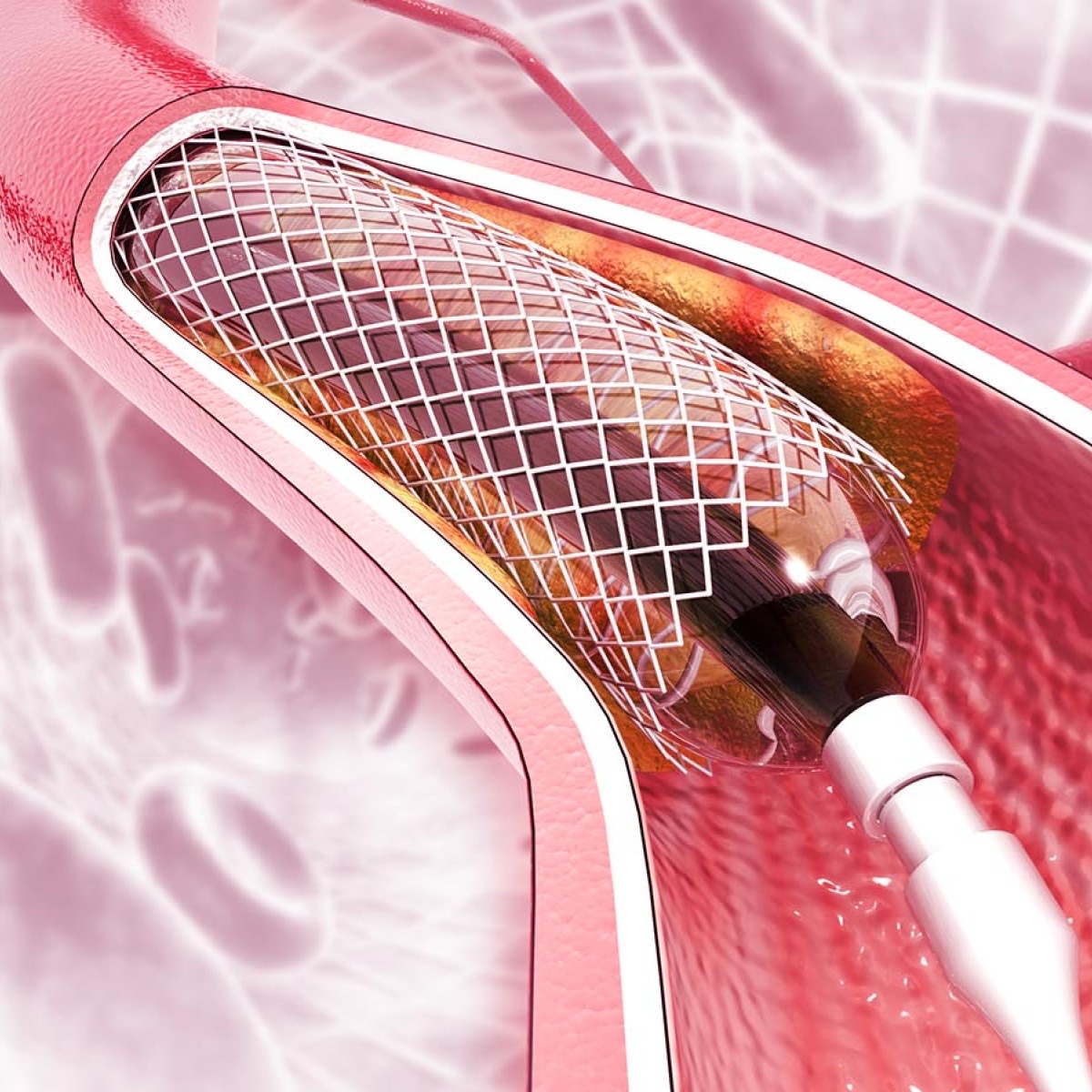
The carotid arteries are the two large blood vessels on either side of the neck that deliver oxygen-rich blood to the brain. Over time, plaque — a buildup of cholesterol, fat, and other substances — can accumulate in the artery walls, causing the vessel to narrow. This condition is called carotid artery disease, or carotid stenosis.
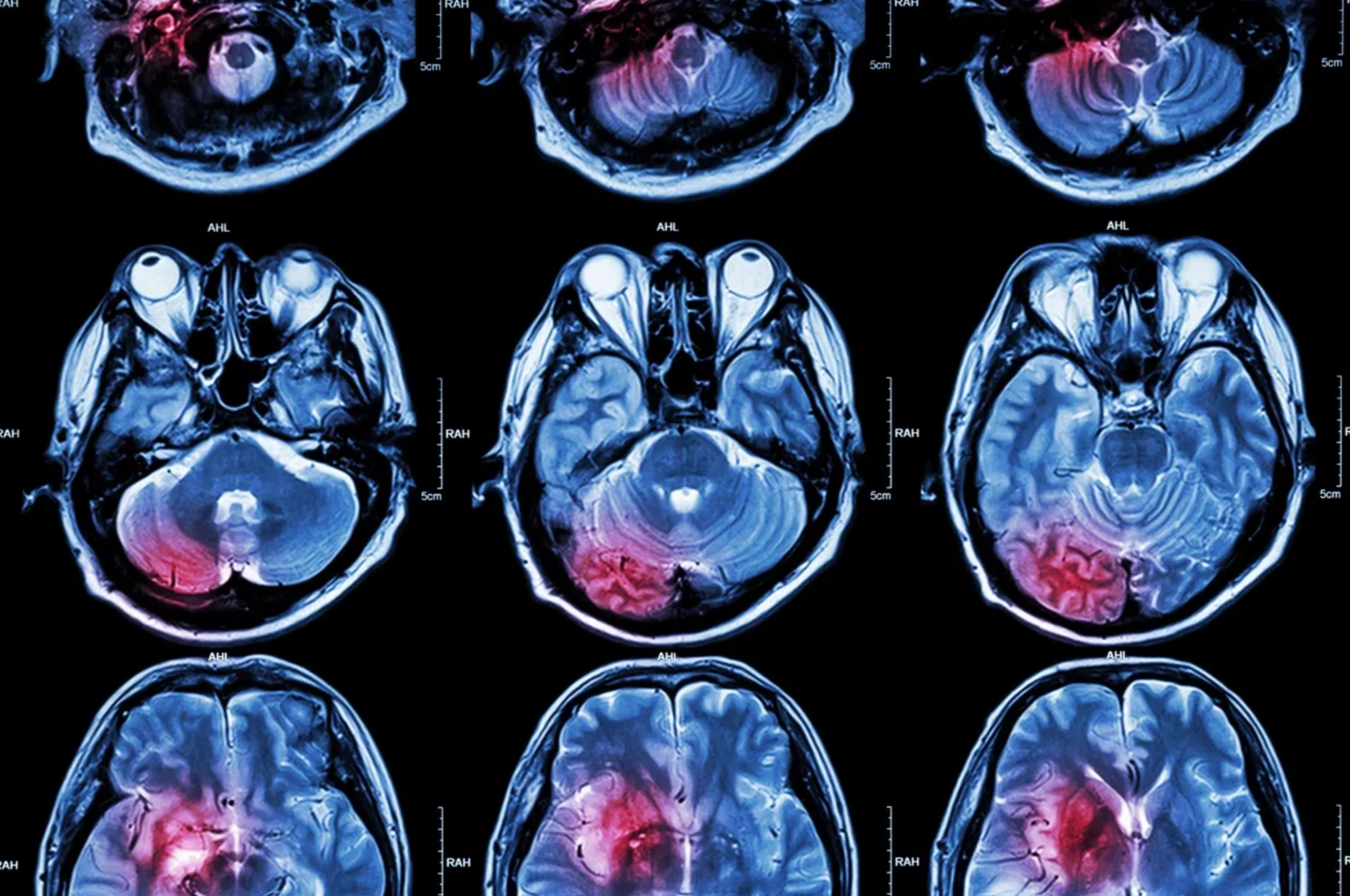
When the carotid arteries become significantly narrowed, the risk of stroke increases substantially. Pieces of plaque can break loose and travel to the brain, or the narrowed artery may block blood flow entirely. Carotid artery disease is one of the most common and treatable causes of stroke.
Vertebral artery disease follows a similar pattern in the vertebral arteries, which supply blood to the back of the brain. Both conditions require careful evaluation and, in many cases, intervention to reduce stroke risk.